Pediatric DKA
By: Yvonne Giunta, MD
For this week, rather than a case, I am going to break down Peds DKA into all the things you may want to know in a quick question/answer format. We see new onset DM in children often. We see known children with DM present in DKA often. They are some of our sickest patients and we need to be really good at this. With that said, I have taken learning points from years (or decades) of cases presented at PI or cases requested for review, and turned it into a learning opportunity for all of us. Further, attached is our very well-known Peds DKA Highlight and Technical Report so you have all the information in one place. At the bottom is a podcast that I think is worth a listen on Peds DKA. Enjoy!
New onset diabetic (in DKA or not).... Anything special I need to do?
Yes! We need to send a whole panel of labs that will eventually be interpreted by peds endocrine, that will help finalize the diagnosis. For example, C peptide, Glutamic Acid Decarboxylase Antibody, Islet Cell antibody. The good news is that you don't have to remember any of that, just go to the order set and select all. These labs need to be collected prior to starting insulin so it is very important that we don't leave this to the inpatient team.
This is the name of the order set:
Peds New Onset Diabetic (Save it to your favorites so it's easier to find when you need it).
What if the patient is not "new onset", but is in DKA, should I still order all those other labs? No. In that case just go to the order set called ED Diabetic Ketoacidosis, Pediatric ( Age 0-18). Save it to your favorites so it's easy to find.
What if I am suspicious of DKA, but not sure,,, what do I do about fluids? The guideline recommends immediate fluid resuscitation with 0.9% NaCl at 10-20 ml/kg over one hour. I personally recommend being cautious and sticking to 10 ml/kg. Can give the bolus faster (5-20min) if the patient is in shock. Before that time is up you will get back the VBG and start adding plenty of fluids, so I would be more cautious up front until you know what your dealing with for sure. If needed you can repeat a bolus once.
OK, the child is in DKA, now what do I do about fluids, what rate am I giving? Keep it simple, just calculate 1 ½ maintenance rate. Know your 4/2/1 rule and calculate the maintenance and then add half = 1 ½ maintenance. If you want to get very technical ( (Maintenance over 48 hours + % Deficit) - Bolus given) divided by 48 hours. I would be happy to go over that with anyone who needs a refresher in person.
Do you ever bolus insulin in peds? No NEVER. Don't do it.
What dose of insulin drip should I start? Typically, we start at 0.1 unit/kg/hr. Sometimes if the patient seems to be very sensitive to insulin, we can start or drop down to 0.05 units/kg/hr.
Do I need to factor in the volume of my insulin drip in my fluid correction? No. It is such a small volume, it does not need to be factored in.
How about LR, can I use that instead of NS? All our recommendations and guidelines (right now) are with NS. For now I would advise sticking with that. However, LR is likely safe and may even be better. It just not as commonly used in Peds so I would recommend going with NS.
When do I need to consider the two-bag method? Always! Especially because it could take some time to make that D10 bag, so order it right away so hopefully it will be ready, and at bedside, if you need to turn it on.
What exactly is the two- bag method? Refer to Table 3 on the HIGHLIGHT attached for full details. But in short, you have 2 bags at the bedside at the same time. Both bags have the same sodium and potassium concentrations. Usually, one bag is 0.9% NS and the other bag is D10 NS. Once you have calculated the 1 1/2 maintenance rate, you will titrate the rate of each bag in order to keep the glucose from dropping too quickly. You will titrate the rate of each bag individually while keeping the total rate the same at 1 ½ Maintenance. (Please note that these 2 bags could be varied based on electrolytes) (Also note that in more dehydrated patients we may give up to 2x maintenance).
When do I start the 2 bag method? When the serum glucose drops below 300 mG/dL.
How fast or slow do you want to drop the glucose? Ideally you do not want to drop > 100 mG/dL/hr. Initially you may see a large drop in glucose associated with the bolus of fluid, but try to not to drop more than > 100 mG/dL/hr.
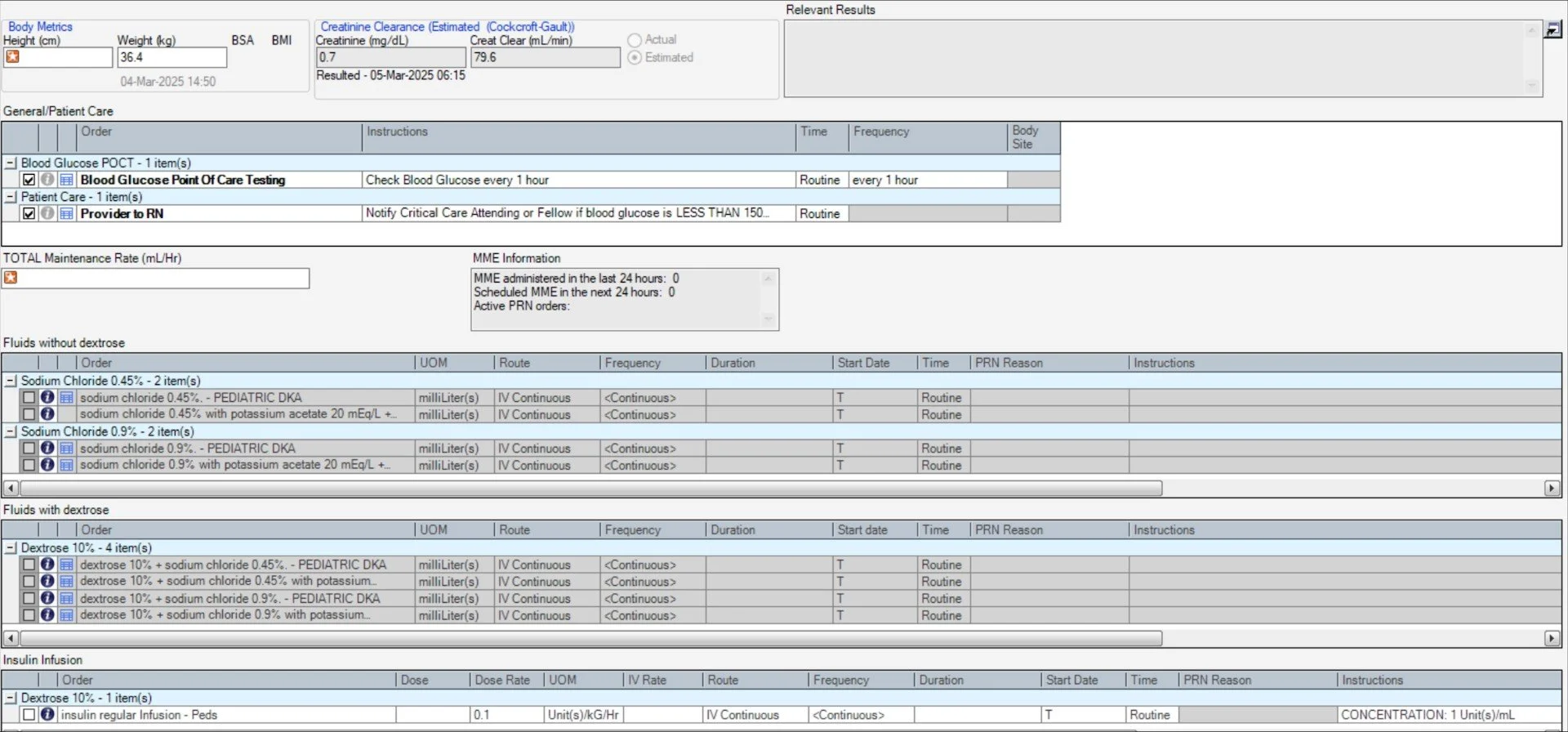
How do I order the 2 bag method?
The order set: DKA IV FLUIDS (0-18) should be what is used (see screenshots) to order the second stage fluids and the insulin infusion. The protocol recommends 1.5-2x maintenance; start with 1.5x and we can go up if necessary. The TWO fluids that must be ordered by the ED STAT are D10W 0.9NS and NS (from this order set). A total fluid rate must be entered first, before choosing the fluids and you must click on both the glucose and non-glucose containing bags. Then the order will nicely calculate the rate of each bag depending on POCT (and in line with the chart on the guideline). The insulin infusion can be ordered from this set as well. If you do not put in the rate at the top, that you calculate (1 ½ maint) you will not be able to place the order.
As already mentioned, the default for the orders is ROUTINE, so you need to change it to STAT. This will make the order a priority in pharmacy. I also follow up the order with a phone call to pharmacy.
What about Potassium? If the potassium is less than 3.3 you must replete the potassium before you give insulin because as soon as you start insulin the potassium will be driven into the cells. Add potassium to the IV fluids once the patient has urinated and the K level is less than or equal to 5.5 mmol/L. Add 40 mEq/L of potassium:
20 mEq/L potassium acetate and 13.6mmol/L (equivalent to 20 mEq/L)
*The potassium is added to both bags in the 2 bag method
OK, I am doing everything right but the repeat blood gas doesn't look good. What do I do now? Check all your math first. Sometimes the initial blood gas looks worse before it looks better. You may just need time. There may be an initial worsening of the acid-base status (fall in pH and HCO3) during the first 1-2 hours of therapy because of the reperfusion of previously under perfused capillary beds and the consequent liberation of lactic acid.
However, make sure that the insulin drip tubing was primed correctly with the insulin drip in the tubing itself and not primed with saline alone. If not primed correctly, when running at such a slow rate, it could take a long time for the insulin to make it to the patient.
How often am I checking labs? Well, hopefully the attending has communicated with the peds intensivist and this patient will go up to PICU expeditiously. However, that is not always the case. In collaboration the PICU senior, remember that we should be checking blood glucose, VBG with electrolytes and neuro-checks hourly and CMP every other hour.
Patient is in DKA but also has a fever..... Find the source of the fever and treat it if you can. The stress of the illness is likely what is making the patient present in DKA. If we don't fix that part, it will be hard to correct the electrolytes overall.
What if the pharmacy is taking forever to send the D10NS, my patient is in DKA, but the glucose is not very high and I'm scared to start insulin without D10NS at bedside? First make sure you ordered as STAT and call the pharmacy. Next, use D5NS instead at double the rate of D10NS, WHILE KEEPING THE TOTAL VOLUME OF FLUIDS THE SAME !!!!!! D5NS is readily available in the ED so you can start this right away, just make sure your math is correct.
Do you ever use 0.45%NaCl? Very rarely, if patients present with hypernatremia or hyperchloremia.
Do you ever use insulin over 0.1 units/kg/hr? Very rarely
Some other pointers:
Don't forget to disconnect their pump (if they have one). Don't just turn it off, take it off them completely if they haven't already. Otherwise, the patient may be getting more insulin than you are aware of.
Make sure you order your D10NS and insulin drip as STAT. This will bump it to the top of the orders for pharmacy to verify. You need to manually change it, it does not default to STAT.
Don't forget to consult Peds Endo on call. They like to know about these patients.
Don't forget to remind the nurse to prime the insulin drip properly. This could make a big difference and it's worth the additional reminder.
You should see a rise in the serum sodium with the lowering of the serum glucose

Click below to view Northwell’s Pediatric DKA pathways and guidelines: