13 yo F with pmhx of "anemia" presents with acute onset vomiting and decrease in po intake. Mom reports pt has been vomiting multiple episodes since yesterday. Denies any abdominal pain. No fevers. No diarrhea and reports having normal bowel movements. Last BM 2 days ago. Mom reports no po intake since yesterday due to nausea and vomiting. At baseline, pt eats "2 foods only, chicken soup and chocolate chip cookies". No dysuria. No back pain. No headaches. Not taking any medications. Further history obtained from mother states that child is undergoing evaluation by neurology for ADHD, which mom states she "meets all of the criteria". Doing poorly in school, does not socialize with friends. Mom also reports that when looking at the vomit, she noticed little strings in it. When she confronted the patient, the patient reports she has been eating strings off the couch pillows for the last 6 months.
Vitals: T98 HR 99 BP 108/72 RR 20 O2 99%on RA Wt 38kg
PE sick appearing, thin, curled in a ball under blankets
HEENT no conjunctiva pallor perrla eomi tm clear pharynx clear mmm
CVS s1 s2 no murmurs
Lungs cta bilaterally
Abd soft ntnd
Ext from x 2
Skin no rashes wwp
What is your initial work up for patient?
Zofran, po trial?
Labs? Imaging?
CBC WBC 10.35 Hgb 10.7 Hct 33.6 plt 309
MVC 75.7
Unremarkable CMP
Iron studies
Iron 37
TIBC 480
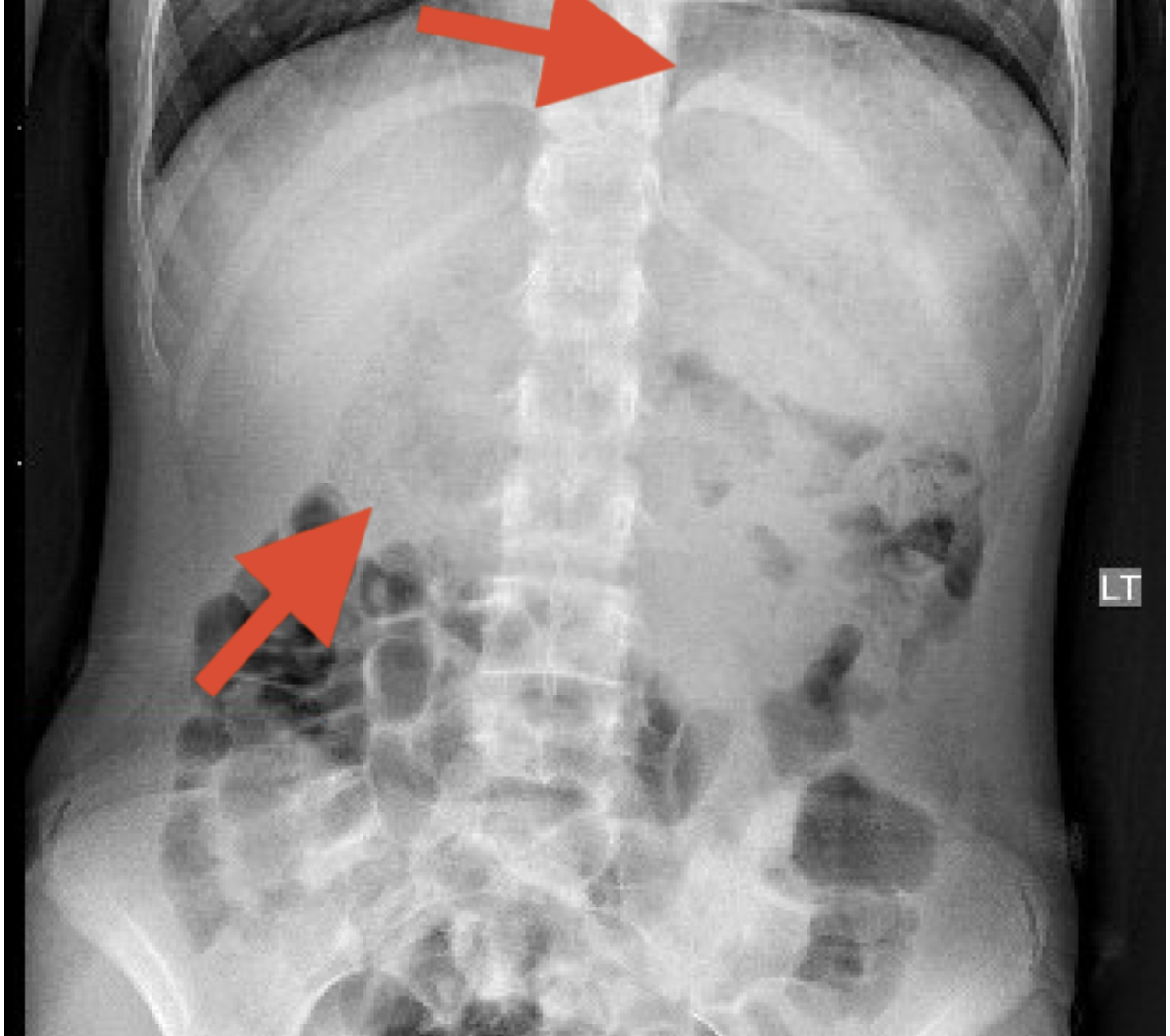
KUB ordered due to hx of possible string ingestion.
Does this XR change your management?
XR read: The stomach is distended with intragastric mottled gas pattern. The entire duodenum is distended with a heterogeneous filling defect which is surrounded by air and extends into the proximal jejunum.
***BEZOAR***
Surgery and GI consulted. CT scan done for further characterization: CT abd/pelvis with oral contrast. Pt drank 1 cup of contrast about 10 mins prior to CT imaging.
Pt was made NPO, IVF, admitted for further management with definitive treatment.
Bezoars are commonly seen in adolescent females and most commonly seen in the stomach.
There is an association with PICA , psychiatric disorders, and developmental delay.
Bezoars are classified into four types:
Phytobezoars-composed of indigestible food particles that are found in vegetable or fruit fibers
Trichobezoars are composed of a conglomeration of hair and food particles
Lactobezoars are composed of milk protein
Pharmacobezoars are concretions of various medications (aluminum hydroxide gel, enteric-coated aspirin, sucralfate, guar gum, cholestyramine, enteral feeding formulas, psyllium preparations, nifedipine XL, and meprobamate)
Management
GI consult for endoscopic removal.. There is a risk of perforation with endoscopic removal. Some bezoars might be too large for endoscopy and surgical removal via laparoscopy might be necessary.
Tama's Tips
Get a good history.
Consider imaging for cases that are deviating from the "usual path"
Know the classic findings of a bezoar on XR
Consider iron deficiency anemia as a cause for PICA
Get psychiatry involved.
PICA
Thank you all
Until next time,
Maria